
Excisional Debridement
Provident has been engaged in ongoing DRG audits since ICD-10 was implemented in October 2015. We have identified potential DRG audit target areas related to our audit work, changes to the ICD-10 codeset, and Coding Clinic updates. We will be posting cases regularly in our newsletter. Please see this edition’s case study below:
Case Summary 1
66-year-old female with extensive prior medical history presents to ED by family for foul-smelling stage IV sacral decubitus ulcer. White count was elevated to 28.4 and she was started on IV antibiotics. She was seen by the Plastic Surgery service and was noted in the Progress Notes to have a, “sacral pressure sore cleansed, necrotic tissue excised and sent for cultures.”
DRG Options
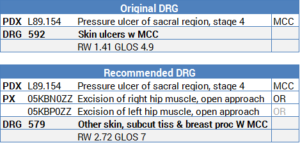
Audit Considerations & Strategies
- The original coder did not code the pressure ulcer excision. Adding either the right or left hip excision would drive the case from a medical DRG (592) to a surgical DRG (579)
- The procedure code may have been overlooked because the surgeon documented that the tissue was “excised” rather than documenting that an “excisional debridement” was performed
- Documentation of “excision” or “excised” is sufficient to code PCS root operation: Excision
- Always carefully review the entire medical record including the Progress Notes for bedside procedures, especially for patients with pressure ulcers (procedures will not always have an Operative Report)
- Per Coding Clinic1, the body part value for an excisional debridement performed on a muscle in the sacral region is the “Hip muscle.” If the documentation specifies that the right side or left side of the sacral ulcer was debrided, then a single code can be assigned. If the documentation does not specify laterality, assign codes for both the right and left hip muscles.
- Since only “excision of sacral pressure sore” was noted, both the 0KBN0ZZ (Excision of right hip muscle) and 0KBP0ZZ (Excision of left hip muscle) codes were assigned
- Coding Clinic likely allows coders to assume both the right and left hip muscles when laterality is not specified because sacral pressure ulcers often develop on the lower back which would include portions of the left and right hips
- Cases with a principal diagnosis of stage 3 or 4 pressure ulcer automatically result in DRG 592: Skin ulcers with MCC (stage 1 or 2 have no impact on the DRG)
- ICD-10 only requires one code to be assigned for the pressure ulcer and stage (ICD-9 required two separate codes)
Reference
- Excisional Debridement of Sacrum Coding Clinic – 3rd Quarter 2016: Page 20
Case Summary 2
76-year-old female with extensive prior medical history including diabetes presents to ED by family with a chronically infected ulcer of the left heel. White count was elevated to 25.2 and she was started on IV antibiotics. She was seen by the Plastic Surgery service and was noted in the Progress Notes to have a, “left heel ulcer, necrotic skin tissue excised and sent for cultures.”
DRG Options
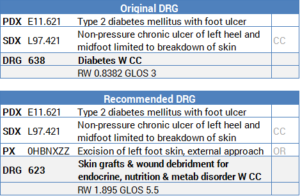
Audit Considerations & Strategies
- The original coder did not code the diabetic foot ulcer excision. Adding the excision would drive the case from a medical DRG (638) to a surgical DRG (623)
- Non-pressure ulcers of the leg (thigh, calf, ankle, heel, midfoot) except the toes are CCs
- The depth of the non-pressure ulcer does not change the CC designation (non-pressure ulcers involving the skin, fat, muscle, bone, or unspecified are all designated as CCs)
- Non-pressure ulcers of the toes, buttocks, back, and other/unspecified sites are not CCs
- ICD-10-CM assumes a causal relationship between diabetes and foot ulcers as well as any condition indented under the word “with” in the Alphabetic Index (i.e. If a patient is admitted with a foot ulcer and has a history of diabetes then a diabetic ulcer should be coded)
References
- Diabetic Foot Ulcer Coding Clinic – 2nd Quarter 2016: Page 12
- Clarification: Diabetes and Associated Conditions Coding Clinic – 2nd Quarter 2016: Page 36