
Provident has been engaged in ongoing DRG audits since ICD-10 was implemented in October 2015. We have identified potential DRG audit target areas related to our audit work, changes to the ICD-10 codeset, and Coding Clinic updates. We will be posting cases regularly in our newsletter. Please see this edition’s case study below:
Case Summary
This is a 77-years-old-female with history of hypertension, type 2 diabetes mellitus, chronic kidney disease stage III, chronic anemia, CAD status post CABG, hypothyroidism, right BKA, and diastolic CHF who was directly admitted to undergo a left fourth toe amputation for osteomyelitis which was successfully performed. Her postop was complicated with profound weakness and fatigue likely secondary to symptomatic acute on chronic blood loss anemia. Baseline hemoglobin level was 8.9 g/dL is which significantly decreased to 6.1 g/dL for which she required transfusion of 2 units of PRBCs leading to an improvement of her hemoglobin level from 6.1 g/dL to 10.2 g/dL. Chronic component of her anemia is likely secondary to CKD stage III. After improvement of her anemia, she was discharged home in stable condition.
DRG Options
Note: Full listing of secondary diagnoses and procdure code assignment not shown
Audit Considerations & Strategies
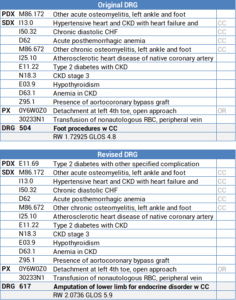
- The coder incorrectly assigned 172 – Other acute osteomyelitis, left ankle foot as the principal diagnosis
- The patient has a history of type 2 diabetes; therefore, the osteomyelitis is assumed to be due to diabetes according to the ICD-10-CM Official Guidelines for Coding and Reporting which changes the principal diagnosis to E11.69 – Type 2 diabetes with other specified complication
- The DRG shifts from 504:Foot Procedures with CC to 617:Amputation of Lower Limb for Endocrine Disorders with CC
- Prior to the Index being revised October 1, 2016, ICD-10-CM did not presume a linkage between diabetes and osteomyelitis; the provider needed to document a linkage or relationship between the two conditions
- With this rule change, all the conditions listed under “Diabetes>with” are assumed to be due to diabetes and should be coded as such
- Conditions such as peripheral arteriosclerosis and peripheral vascular disease in a diabetic are assumed to be due to diabetes and therefore should be captured with 51- diabetes with diabetic peripheral angiopathy
- The only exceptions to this rule are conditions that include “NEC” (not elsewhere classified) in their description (e.g. E11.628 – Skin complication NEC, E11.618 – Type 2 diabetes with other diabetic arthropathy)
- For example, if a patient with a history of diabetes is admitted with cellulitis, the cellulitis is not assumed to be due to diabetes since cellulitis is not listed under “Diabetes>with” in the ICD-10-CM Index (only skin complication NEC is listed)
- If it is unclear whether the cellulitis is related or unrelated to diabetes, a query should be sent to the provider for clarification.
- If the cellulitis is found to be related to diabetes, then the principal diagnosis would be E11.628 – Diabetes with other skin complications followed by a code for the cellulitis
- Whenever reviewing/coding charts where patients have a history of diabetes, always make sure to assign the appropriate diabetic complication code followed by a code for the complication except for complications including NEC in their description
- Ensuring that the appropriate diabetic complication code is assigned and sequenced accurately can significantly impact the DRG assignment
- Whenever it is unclear whether or not a condition is related to diabetes, query the provider for clarification
References
- AHA Coding Clinic, 2nd Quarter 2018: Page 7 – Diabetes with Peripheral Angiopathy
- AHA Coding Clinic 4th Quarter 2016: Page 118 – Changes to the ICD-10-CM Official Guidelines for Coding and Reporting
- AHA Coding Clinic, 1st Quarter 2016: Page 11 – Diabetes with Associated Conditions