
Provident has been engaged in ongoing DRG audits since ICD-10 was implemented in October 2015. We have identified potential DRG audit target areas related to our audit work, changes to the ICD-10 codeset, and Coding Clinic updates. We will be posting cases regularly in our newsletter. Please see this edition’s case study below:
Case Summary
This is a 69-year-old male brought to the trauma center after sustaining a crushing injury when the horse he was riding slipped in the mud, threw him off and then landed on top of him. The patient had positive loss of consciousness with decreased sensation and movement of all his extremities at the scene. The patient was evaluated and found to have C3 through L5 stenosis and central cord syndrome. Neurosurgery was consulted. They recommended an MRI and after review of his scans, planned operative fixation of spine.
Postoperatively, the patient did well with noted acute blood loss anemia. His neuro exam continued to improve with no deficits to his bilateral lower extremities. He was deemed stable for discharge to rehabilitation.
Operative Procedures:
- C3 through C6 posterior segment instrumentation and fusion
- C3 through C6 posterolateral fusion
- C3, C4 and C5 complete laminectomies
DRG Options
Note: Full listing of secondary diagnoses and procdure code assignment not shown
Audit Considerations & Strategies
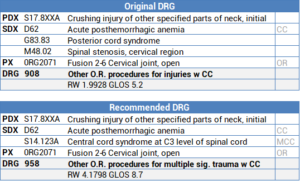
- The coder correctly assigned the principal diagnosis as S17.8XXA – crushing injury of other specified parts of neck, initial encounter
- 0RG2071 was correctly assigned for the fusion
- However, the coder incorrectly assigned G83.83 – posterior cord syndrome for the central cord syndrome (there is no G83 code for central cord syndrome)
- Following the ICD-10-CM Index: Syndrome > Cord directs coders to two codes:
- 82 – anterior cord syndrome or
- 83 – posterior cord syndrome
- The excludes1 note under the G83.8 – other specified paralytic syndromes states:
- Paralytic syndromes due to current spinal cord injury – code to spinal cord injury (S14, S24, S34)
- Based on the Excludes1 note, following the Index: Injury>spinal>cervical (neck)>central cord syndrome>C3 level takes the coder to 123A – central cord syndrome at C3 level of cervical spinal cord
- The instructional note under the S14 sections states, “Code to highest level of cervical cord injury”, therefore only a code for the C3 injury is necessary
- Replacing G83.83 posterior cord syndrome with S14.123A central cord syndrome at C3 level drives the DRG from 908 Other O.R. procedures for injuries w CC to 958 Other O.R. procedures for multiple significant trauma w CC
- Recommend removing M48.02 – spinal stenosis, cervical region since this is a traumatic injury
- Whenever coding trauma cases make sure to assign codes for the current spinal cord injuries (acute) rather than the primary progressive (chronic) syndromes because of the significant DRG implications
- Cord Syndrome definitions:
- Central cord syndrome is an incomplete traumatic injury to the cervical spine resulting in more extensive motor weakness in the upper extremities than the lower extremities. The mechanism of injury occurs from a forceful hyperextension neck injury with prior existence of degenerative ligamentous and osteophytic spinal column disease. There is usually no obvious associated spinal column fracture or evidence of spinal instability.
- Anterior cord syndrome results from injury to the motor and sensory pathways in the anterior parts of the spinal cord. These patients can feel some types of crude sensation via the intact pathways in the posterior part of the spinal cord, but movement and more detailed sensation are lost.
- Posterior cord syndrome results from the bilateral involvement of the dorsal columns, the corticospinal tracts (CSTs), and descending central autonomic tracts to bladder control centers in the sacral cord. Dorsal column symptoms include gait ataxia and paresthesias. CST dysfunction produces weakness that, if acute, is accompanied by muscle flaccidity and hyporeflexia and, if chronic, by muscle hypertonia and hyperreflexia. Extensor plantar responses and urinary incontinence may be present.
- Causes of a dorsal cord syndrome include multiple sclerosis (more typically the primary progressive form), tabes dorsalis, Friedreich ataxia, subacute combined degeneration, vascular malformations, epidural and intradural extramedullary tumors, cervical spondylotic myelopathy, and atlantoaxial subluxation.
References
- American Association of Neurological Surgeons, https://www.aans.org/Patients/Neurosurgical-Conditions-and-Treatments/Central-Cord-Syndrome, https://www.aans.org/Patients/Neurosurgical-Conditions-and-Treatments/Spinal-Cord-Injury
- UpToDate, https://www.uptodate.com/contents/anatomy-and-localization-of-spinal-cord-disorders