
Getting to Know Core Measure SEP-1: Early Management Bundle, Severe Sepsis/Septic Shock
The new CMS Core Measure for sepsis (SEP-1) has drawn praise, criticism, and confusion. Providers, documentation specialists, and coders need to collaborate to ensure sepsis is properly documented and treated to ensure compliance with CMS Core Measure SEP-1.
Effective October 1, 2015, CMS began requiring hospitals to collect data for Core Measure SEP-1: Early Management Bundle, Severe Sepsis/Septic Shock (See chart below). According to CMS, “The purpose of the Severe Sepsis and Septic Shock Early Management Bundle measure is to facilitate the efficient, effective, and timely delivery of high quality sepsis care in support of the Institute of Medicine’s aims for quality improvement. By providing timely, patient-centered care and making sepsis care more affordable through early intervention, this measure can result in reduced use of resources and lower rates of complications.”
As reported by Joyce Frieden in MedPage Today, “The new federal reporting requirements for treating hospitalized sepsis patients has drawn both praise and criticism from physicians who treat the condition.”
- “The intent of the measure is good,” said Scott Weingart, MD, an emergency physician at the State University of New York at Stony Brook. “When you look at it, you could argue this is going to help, in that it will add more recognition [to the problem]. … but it’s always about not knowing the unintended consequences.”
- Weingart continued to say that “They have re-dubbed severe sepsis to be something very different than we are used to or have read in any of the major sepsis studies … I am still fairly desperate to know the evidence for this new definition, but I haven’t found it yet. Pretty unacceptable to hold every hospital in the U.S. accountable to an arbitrary definition that has not been tested in large-scale trials.”
- “Christopher Seymour, MD, of the University of Pittsburgh School of Medicine, said in a phone interview that because sepsis is a syndrome, “There is no single characteristic that identifies septic patients, and that’s what makes it such a challenge.” However, he added, “Sepsis is under recognized and underdiagnosed, and anything we can do to promote doctors and hospitals to take better care of patients with sepsis is serving the greater good.”
- Ronald Nahass, MD, chair of the quality committee at the Infectious Diseases Society of America (IDSA), said in a phone interview that IDSA “applauds the fact that [CMS is] looking at it and trying to address it as a problem — because it is. It has a huge cost.”
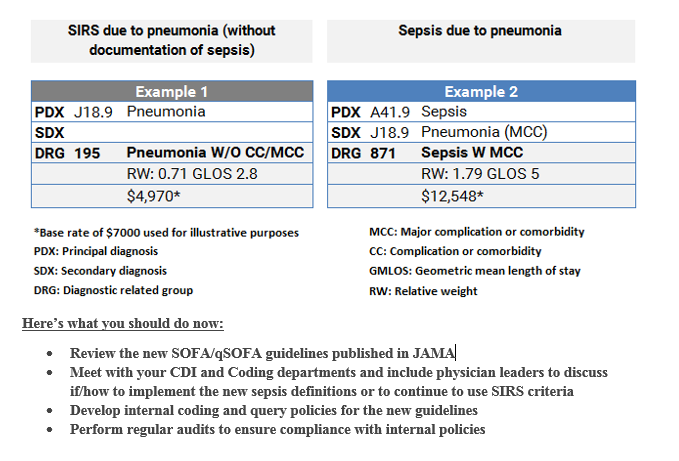
Properly diagnosing and treating sepsis will likely become an even greater task now with the recently released SOFA (Sequential Organ Failure Assessment) and qSOFA (Quick SOFA) clinical criteria for diagnosing sepsis and septic shock published in the Journal of the American Medical Association (JAMA February 23, 2016).
CMS defines severe sepsis as “having a suspected source of clinical infection and two or more manifestations of systemic infection (SIRS criteria) plus one or more variable of organ dysfunction”. SIRS criteria include:
- Temperature >38.3 C or <36.0 C
- Heart rate >90 beats per minute
- Respiration > 20 breaths/min
- White blood cell count >12,000 or <4000/mm3, or >10% bandemia
With the increased focus on properly reporting sepsis, there is an even greater need for providers, quality and clinical documentation specialists, and coders to collaborate to ensure sepsis is consistently documented, coded, and reported. Providers, coders, and CDI specialists, need to collaborate to decide whether to follow the current SIRS definition for sepsis or to use the new SOFA criteria for coding and reporting purposes. The SOFA criteria is stricter than the SIRS criteria, which should lead to a decrease in the number of patients diagnosed with sepsis. Whether the current SIRS or the new SOFA definitions are used to diagnosis sepsis, to comply with the requirements of SEP-1, hospitals must adhere to the sepsis treatment bundles. Information on the sepsis bundles are outlined below as well as an example of the financial impact of documenting SIRS versus sepsis.
Hospital documentation policies for sepsis have real world financial impacts
Severe Sepsis
Within three hours of presentation
• An initial lactate level measurement must be obtained. If the results are >4mmol/L, resuscitation with 30ml/kg crystalloid fluids should be started
• Blood cultures drawn prior to antibiotic administration
• Broad spectrum or other antibiotics must be administered
Within six hours of presentation
• Repeat lactate level measurement should be done if the initial lactate measurement was elevated (> 2mmol/L).
Septic Shock
Within three hours of presentation
• In addition to the severe sepsis interventions, start resuscitation with 30ml/kg crystalloid fluids for hypotension or lactate >= 4 mmol/L
Within six hours of presentation
• If hypotension (systolic blood pressure (SBP) < 90 mmHg or mean arterial pressure (MAP) <65mmHg) persists after fluid administration, the following treatments must be initiated:
• Vasopressor administration
• Repeat volume status and tissue perfusion assessment by completing one of the following:
1. Option 1: Document a focused physical exam including:
o Vital signs, cardiopulmonary exam, capillary refill evaluation, peripheral pulse evaluation, and skin examination
2. Option 2: Document two of the following:
o Central venous pressure measurement
o Central venous oxygen measurement
o Bedside cardiovascular ultrasound
o Passive leg raise or fluid challenge
Hospital documentation policies for sepsis have real world financial impacts
Example of financial impact of documenting sepsis versus SIRS
Related Links
- CMS Sepsis Measures Spark Controversy
- The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3)
- Do you know the new Sepsis Criteria?